Abstract
Keywords: Poly-γ-glutamic acid; deciduous teeth; remineralization; demineralization; dental caries; biomimetic material
Dental caries remains a major global health problem primarily driven by bacterial acids and it is a common disease among children. It causes enamel and dentin of teeth to lose minerals [1]. The prevalence of dental caries among young children is very high. Caries occurrence has been reported to be up to 71.9% in 5-year-old children in some areas. This means there is a need for better preventive and therapeutic approaches, as restoration only is not enough. Besides that, children are seen to develop caries rapidly, and that is why the limited care options to stop caries progression are not enough [2]. This urgent problem has led to a lot of research in new biomaterials and minimally invasive approaches to stop demineralization and encourage remineralization of the earliest stages of caries, which is still a big problem especially in deciduous teeth where caries tend to progress rapidly [3]. For example, bioactive restorative materials are attracting more attention because they are able to release fluoride, calcium, and phosphate ions, which in turn help to remineralize the neighboring carious lesions [4]. One biomaterial that is receiving a lot of attention as a possible candidate is poly-γ-glutamic acid (PGGA). It is a natural, biodegradable polypeptide with chelating and mineral-binding properties that make it highly effective in remineralization processes [2].
Pharmaceutical-grade fluoride remains the most effective, widely-used and trusted dental health product; however, if absorbed inappropriately it can lead to toxicity symptoms such as nausea vomiting abdominal pain, diarrhea, and excessive salivation. This is why developing a potent, safe and biocompatible drug for children is still one of the most important research goals. PGA can also play a key role in enamel repair by stabilizing calcium and phosphate ions and subsequently promoting hydroxyapatite crystal formation as its polymer structure allows it to chelate metal ions [5].
The purpose of the present work was to examine the potential of PGGA acid treatment in protecting enamel by both reducing the rate of release of minerals and encouraging remineralization in primary teeth, that is why we are seeking an efficient material for caries treatment in pediatric dentistry. In detail, the goal of this paper is to analyse the impact of different PGGA concentrations alone and combined with the addition of hydroxyapatite on artificial caries lesions in primary teeth under the shell of simulated oral conditions. The experimental setup for this research will be a pH cycling model that reproduces ‘both sides of the coin’—demineralization and remineralization phases—a necessary condition for the oral environment that is usually ignored in studies that use static models [6,7].
2.1. Preparation of solutions and specimens
Stock solutions of 0.1 M acetic acid, sodium fluoride (NaF), and PGGA were freshly prepared and stored in sterile Thomas PP narrow-mouth bottles (Thomas Scientific, UK). All containers were autoclaved at 121°C and 15 psi for 15 min to maintain sterility and avoid microbial growth.
The 0.1 M acetic acid demineralizing solution was adjusted to pH 4.0 using a 1 M NaOH solution, and the final pH was verified with a calibrated pH meter [8]. Phosphate-buffered saline (PBS) was prepared according to the manufacturer’s instructions (Oxoid, UK) by dissolving one tablet in 100 mL of deionized water. The solution was then autoclaved at 121°C for 10 min, its pH was corrected to 7.0 with NaOH, and it was used as the negative control.
PGGA, sourced from Poly-glu (Japan), was prepared at 1% and 2% (w/v) concentrations using deionized distilled water. Both formulations were adjusted to pH 7.0 to ensure stability. To promote mineral interaction, 2% hydroxyapatite (HAp) crystals (Plasma Biotal, UK) were added to each PGGA solution. The mixtures were stored at room temperature in sterile, airtight containers until required.
Sodium fluoride solutions at 0.1% and 0.5% (w/v) were prepared in deionized water and adjusted to pH 7.0 using the previously prepared 1 M NaOH. These concentrations were selected because they are commonly used in dental products and served as the positive control.
Ethical approval for the research was granted by the Riyadh Elm University Ethics Committee (FRP/2026/610/1474). A total of 25 sound primary human incisors were collected from patients at the Riyadh Elm University Dental Hospital after obtaining written informed consent. Any remaining soft tissue was removed by gentle scaling, and the teeth were rinsed thoroughly with distilled water before being stored in PBS at room temperature. No pre-treatment—such as acid etching or artificial demineralization—was performed before the experimental procedures.
The sample size was calculated prior to starting the study. Sample size calculation:
A minimum sample size was calculated to estimate the mean calcium loss with 95% confidence (Z = 1.96). Using an expected standard deviation of σ = 0.40 (from pilot readings) and an allowable margin of error of d = 0.36, the sample size was:
Thus, 5 teeth were included in the experimental group.
2.3. Experimental design: assessment of de-/re-mineralization
To assess how PGGA and NaF influence enamel demineralization and remineralization, 25 primary incisors were coated with nail varnish, leaving a 2 × 2 mm2 exposed window on the mid-labial surface to serve as the treatment area. The teeth were then randomly allocated into five groups (n = 5):
(i) 0.1 M acetic acid (negative control),
(ii) 1% PGGA + 2% HAp,
(iii) 2% PGGA + 2% HAp,
(iv) 0.1% NaF, and
(v) 0.5% NaF.
During the demineralization phase, all solutions were kept at pH 4.0. Each specimen was submerged in 0.1 M acetic acid for 24 h to create early enamel lesions. Calcium ion release was recorded every 15 min using a calcium ion-selective electrode (Ca2+ ISE).
Following demineralization, the teeth were placed in their assigned treatment solutions (PGGA + HAp or NaF, adjusted to pH 7.0) for 5 min. They were then transferred back into a mildly buffered acetic acid solution, adjusted to pH 6.0 with 1 M NaOH, for an additional 24 h to mimic remineralization conditions. Calcium ion concentrations were again measured, and the rates of mineral loss or gain were determined through linear regression. A positive slope indicated continued demineralization, whereas a negative slope reflected mineral uptake. The same specimens were later subjected to microhardness testing.
2.4. Scanning electron microscopy (SEM) analysis
The 2 × 2 mm2 uncoated window on the mid-labial surface as the test site was scanned before (after demineralization at pH 4.0) and at the end of the experiment (remineralization at pH 6.0). Prior to the analysis the specimens were air-dried. Each sample was fixed on aluminum pin mounts to hold the specimen. Later same amount was used after treatment at pH 6.0 for the respective samples in order to maintain the position and location for pre- and post-treatment analysis.
2.5. Cross-sectional microhardness (CSMH) analysis
After completing the ion analysis, each tooth was thoroughly rinsed with deionized water. The primary teeth were then sectioned longitudinally through the lesion area using a precision diamond saw. Each half was embedded in epoxy resin so that the lesion surface remained exposed for cross-sectional microhardness assessment [8].
Cross-sectional microhardness (CSMH) was measured following the method originally described by Featherstone et al. [8], with a slight modification. Instead of the standard 50-µm spacing, indentations were placed at 25-µm intervals from the outer enamel surface to a depth of 250 µm. At each depth point, five indentations were made using a 25-g load with a 5-s dwell time. Mineral volume percentages were calculated for every depth, and the relative mineral recovery was determined by integrating the mineral content–depth profile using Simpson’s rule, expressed as volume percent × enamel depth (µm). The finer 25-µm spacing was specifically chosen to better detect subtle subsurface remineralization changes in the PGGA-treated specimens.
As the pH of the various acetic acid solutions was increased from 4.0 to 6.0 in the five acidi-fied treatment groups, the negative values for calcium ions with teeth indicated ion uptake by the teeth for the treatment groups in the following order: Calcium ion uptake rates (increasingly negative RCa2+ values) were in the following order: Acetic acid (lowest) < 0.5% NaF < 0.1% NaF < 1% PGGA < 2% PGGA (highest). Nevertheless, the calcium ion uptake through the teeth in the acidified treatment groups was estimated for RCa2+ through linear regression analysis and are shown in Table 1.
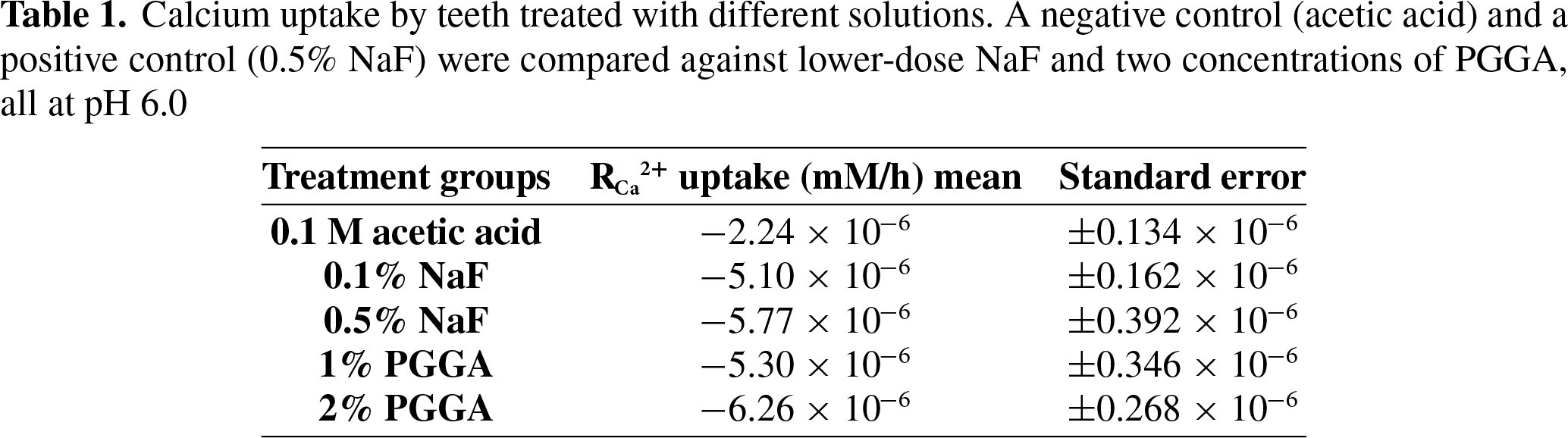
The Z-test was used to analyze the RCa2+ uptake. It allowed for the statistical comparison of different treatment groups with a threshold of ρ < 0.05 for significance. The difference between the negative control and the four treatment groups was statistically signifi-cantly different (Table 1).
The calcium uptake rates (Mean ± SE, n = 5) demonstrated that most treatment groups showed statistically distinct outcomes (ρ < 0.05) during the second 24-h period. The sole exception was between 0.1% NaF and 1% PGGA, which were not significantly different from each other. Acetic acid and the two NaF concentrations served as the negative and positive controls, respectively.
The surface of teeth were later analyzed under SEM before treatment after demineralization at pH 4.0 and post treatment with the positive control 0.5% NaF (B) and experimental groups (2% PGGA (A) and 1% PGGA (C)) as shown in Figure 1. The teeth treated with 2% PGGA showed the paramount surface mineral deposition.

Figure 1. Scanning electron microscopic images of the tooth surface enamel on demineralization with pH 4.0 and later at pH 6.0. (A) Represent the teeth treated with 2% PGGA; (B) teeth treated with 0.5% NaF and (C) tooth treated with 1% PGGA solution
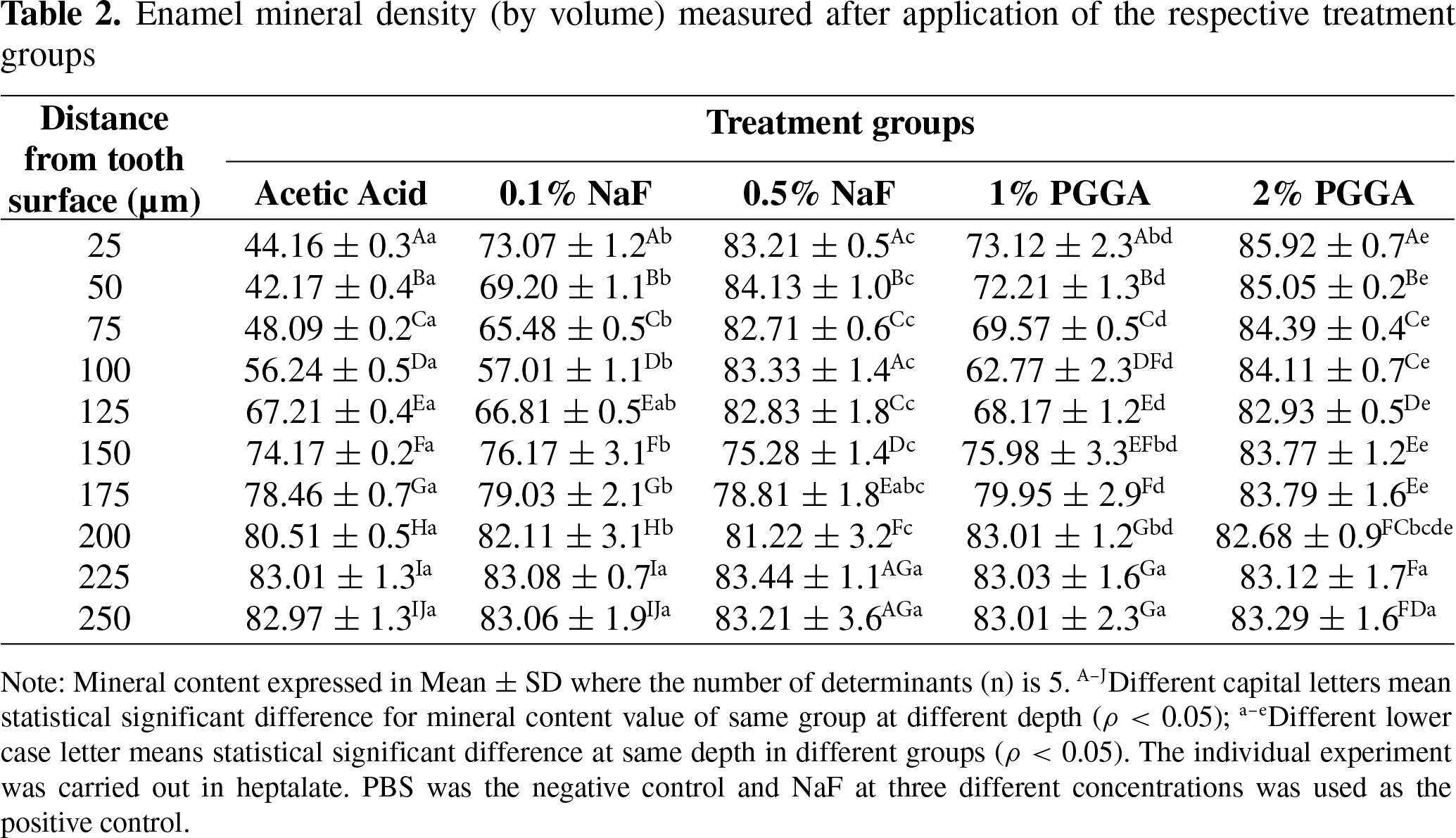
The CSMH of the teeth treated with various solutions at the end of the experiment with pH 6.0 acetic acid solution was evaluated at 25 µm in order to evaluate sub-surface remineralization. The 2% PGGA treated teeth in Table 2 have shown a strong potential for a sub-surface remineralization trailed by the gold standard solution of 0.5% NaF which extended upto the depth of 125 µm (ρ < 0.05). Whereas the sub-surface complete subsurface mineral recovery was not observed for the teeth treated 0.1% NaF and 1% PGGA.
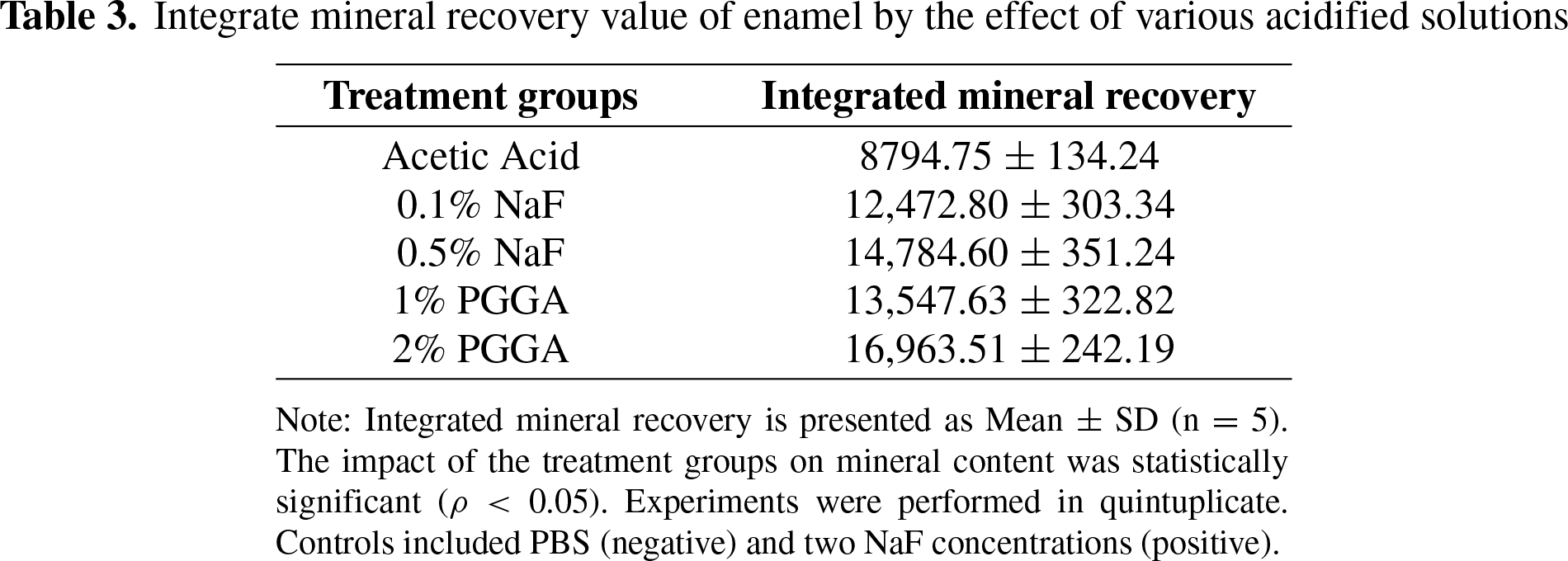
The data in Table 3 quantify the recovery of integrated mineral content in enamel following treatment with various acidified solutions. The results indicate that 2% PGGA was the most effective agent for promoting mineral recovery, whereas 0.1% NaF yielded the lowest recovery. A one-way ANOVA revealed a statistically significant difference in mineral recovery among the treatment groups (ρ < 0.05).
Fluoride is considered as a benchmark treatment option, but due to its limitation and adverse effects for being used by the toddlers there is an emerging need for a biocompatible and biosafe material. The present study evaluated the potential of PGGA as a natural food derivative to inhibit demineralization and promote remineralization in deciduous teeth, contrasting its effects with established fluoride treatments [9]. Our findings indicate that PGGA, particularly at higher concentrations, exhibits superior remineralization capabilities compared to certain fluoride concentrations, aligning with recent advancements in dental material science aimed at enhancing restorative outcomes [10]. This aligns with broader research suggesting that novel biomaterials can provide effective alternatives or adjuncts to traditional fluoride-based therapies for dental hard tissue repair [11]. The observed trends in RCa2+ uptake and integrated mineral recovery suggest a dose-dependent effect for PGGA, where higher concentrations yielded more favorable results in mitigating demineralization and promoting enamel repair. This efficacy potentially stems from PGGA’s chelating properties and its capacity to stabilize calcium and phosphate ions, thereby facilitating their deposition onto the demineralized enamel surface and enhancing the formation of hydroxyapatite crystals [10,12]. Such biomimetic remineralization strategies, which involve crystal nucleation on demineralized enamel, are increasingly recognized for their ability to restore the hierarchical microstructure of enamel [13,14].
Moreover, this biomimetic approach offers advantages over simple ion deposition by fostering structured crystal growth, which is crucial for restoring the mechanical integrity and acid resistance of the demineralized enamel [15]. The nuanced mechanism likely involves PGGA’s ability to create a supersaturated environment of mineral ions while simultaneously acting as a scaffold for organized crystal growth, distinguishing its action from mere precipitation [16]. The incorporation of hydroxyapatite crystals into the PGGA formulations further augmented the remineralization process by providing nucleation sites, thereby accelerating crystal growth and mineral deposition within the enamel matrix, an approach supported by studies on other biomimetic agents [10,14]. The possible reason of PGGA outperforming 0.5% NaF formulation could be the polymeric structure binding larger number of Ca ions and promoting the apatite crystal formation at a faster rate than the positive control (0.5% NaF). The anionic –COOH group present in each glutamic acid residue possesses the ability to react with and bind to the cationic entity of another molecule or biopolymer, or it may act as or remain a free carboxylic acid. Consequently, PGGA acid is capable of dissolving especially Ca and Mg compounds to form stable ionic complexes [17]. In airways of the oral cavity displaying supersaturation, different free ions can be caught by PGGA, in particular the free Ca2+ which at pH conditions lower than those at which statherin is present can still bind and enhance remineralization. PGGA to the same extent as dental caries causing microbial flora (streptococcus mutans) it can resist by secreting a protective layer against the microbe. It can also resist the hydrolytic action of proteases [17,18]. This integrated strategy offers a promising pathway for pediatric dentistry, providing a non-toxic and biocompatible alternative to conventional fluoride treatments [19]. Future research should explore the long-term stability and clinical applicability of PGGA-based formulations in vivo, considering factors such as salivary flow, oral microbiome, and dietary influences on their sustained efficacy. PGGA being an extract of food product, shows potential to be used in various tropical options such as mouthwash, toothpaste and specially as an artificial saliva to protect the teeth from demineralization due to erosion or dental caries.
The findings from this study confirm that PGGA holds considerable promise as a natural, food-derived agent for combating dental demineralization and promoting enamel remineralization in deciduous teeth. Its demonstrated capacity to enhance mineral recovery and facilitate the structural repair of demineralized enamel suggests its potential as a valuable adjunct or alternative to conventional fluoride therapies, especially given its natural origin and biocompatibility.
Acknowledgement: The study was funded and supported by the College of Medicine and Dentistry, Riyadh Elm University, Riyadh, Saudi Arabia. The study is the continuation of the previous studies conducted under the supervision of Prof. Robert Hill and Prof. Paul Anderson at the Queen Mary University of London, London, United Kingdom followed by Prof. Zubaidah Binti Haji Abdul Rahim and Dr. Hooi Pin Chew at the University of Malaya, Kuala Lumpur, Malaysia.
Funding Statement: The study was funded and supported by the College of Medicine and Dentistry, Riyadh Elm University, Riyadh, Saudi Arabia.
Author Contributions: Conceptualization: Zeeshan Qamar, Nishath Sayed Abdul. Methodology: Zeeshan Qamar, Nedal Abu-Mostafa, Abdulkarim Basha. Investigation: Nishath Sayed Abdul, Moaath Ahmad Alsayegh, May Mohammed Alshemaisi, Rahaf Abdurhman Almobty, Basma Yahya. Formal analysis: Zeeshan Qamar, Oubada Suliman. Resources: Abdulkarim Basha, Omar Mohammed Yousef Aleidi. Data curation: Moaath Ahmad Alsayegh, May Mohammed Alshemaisi. Writing—Original draft preparation: Nishath Sayed Abdul, Zeeshan Qamar. Writing—Review & Editing: Zeeshan Qamar, Nedal Abu-Mostafa, Abdulkarim Basha. Visualization: Oubada Suliman. Supervision: Zeeshan Qamar. Project administration: Zeeshan Qamar. Funding acquisition: Zeeshan Qamar. All authors reviewed and approved the final version of the manuscript.
Availability of Data and Materials: Data is available on request.
Ethics Approval: The ethical approval was obtained from the Institutional Review Board of the Riyadh Elm University, Riyadh, Saudi Arabia (FRP/2026/610/1474). The study was conducted in accordance with the local legislation and institutional requirements. The participants provided their informed consent to participate in this study.
Conflicts of Interest: The authors declare no conflicts of interest.
How to Cite this Article
References
- Almishkhas SI, Rasheed Almutairi M, Salem Baazeem R, Sulaimani OM, Alwadi MA, Alkhadra SS, et al. The preventive role of fluoride in dental caries management: mechanisms, efficacy, and clinical applications. Saudi J Med Public Health. 2025;2(1):1–11. doi:10.64483/jmph-21. DOI
- Su QQ, Zhang C, Mai S, Lin HC, Zhi QH. Effect of poly (γ-glutamic acid)/tricalcium phosphate (γ-PGA/TCP) composite for dentin remineralization in vitro. Dent Mater J. 2021;40(1):26–34. doi:10.4012/dmj.2019-324; 32779606 DOI
- Bar-Hillel R, Feuerstein O, Tickotsky N, Shapira J, Moskovitz M. Effects of amorphous calcium phosphate stabilized by casein phosphopeptides on enamel de- and remineralization in primary teeth: an in vitro study. J Dent Child. 2012;79(1):9–14. doi:10.1111/j.1365-263x.2011.01135.x; 21631614 DOI
- Phyo WM, Saket D, da Fonseca MA, Auychai P, Sriarj W. In vitro remineralization of adjacent interproximal enamel carious lesions in primary molars using a bioactive bulk-fill composite. BMC Oral Health. 2024;24(1):37. doi:10.1186/s12903-023-03814-1; 38185656 DOI
- Yuan R, Zhang Y, Liao L, Ge Y, Li W, Zhi Q. Biomineralization-inspired anti-caries strategy based on multifunctional nanogels as mineral feedstock carriers. Int J Nanomed. 2023;18:4933–47. doi:10.2147/IJN.S418465; 37693886 DOI
- Kharbot B, Askar H, Gruber D, Paris S. Biomimetic remineralization of artificial caries lesions with a calcium coacervate, its components and self-assembling peptide P(11)-4 in vitro. Bioengineering. 2024;11(5):465. doi:10.3390/bioengineering11050465; 38790332 DOI
- Myanmar K, Inoue G, Chen X, Shimada Y. Remineralization effects of zinc-containing glass ionomer cement restoratives on demineralized enamel under pH cycling conditions. Crystals. 2025;15(4):329. doi:10.3390/cryst15040329. DOI
- Featherstone JDB, Barrett-Vespone NA, Fried D, Kantorowitz Z, Seka W. CO2 laser inhibition of artificial caries-like lesion progression in dental enamel. J Dent Res. 1998;77(6):1397–403. doi:10.1177/00220345980770060401; 9649168 DOI
- Orsini G. In vitro investigation of the effect of different remineralizing agents on human enamel. Mod Approaches Dent Oral Health Care. 2020;4(3):369–75. doi:10.32474/madohc.2020.04.000189. DOI
- Vitiello F, Tosco V, Monterubbianesi R, Orilisi G, Gatto ML, Sparabombe S, et al. Remineralization efficacy of four remineralizing agents on artificial enamel lesions: SEM-EDS investigation. Materials. 2022;15(13):4398. doi:10.3390/ma15134398; 35806523 DOI
- Damian LR, Dumitrescu R, Alexa VT, Focht D, Schwartz C, Balean O, et al. Impact of dentistry materials on chemical remineralisation/infiltration versus salivary remineralisation of enamel—In vitro study. Materials. 2022;15(20):7258. doi:10.3390/ma15207258; 36295323 DOI
- Akbeyaz Şivet E, Kargül B. Remineralization of artificial caries lesions using casein phosphopeptide-amorphous calcium phosphate containing probiotic lozenge: an in vitro study. BMC Oral Health. 2025;25(1):1086. doi:10.1186/s12903-025-06352-0; 40611049 DOI
- Lv X, Yang Y, Han S, Li D, Tu H, Li W, et al. Potential of an amelogenin based peptide in promoting reminerlization of initial enamel caries. Arch Oral Biol. 2015;60(10):1482–7. doi:10.1016/j.archoralbio.2015.07.010; 26263536 DOI
- Sakr AH, Nassif MS, El-Korashy DI. Amelogenin-inspired peptide, calcium phosphate solution, fluoride and their synergistic effect on enamel biomimetic remineralization: an in vitro pH-cycling model. BMC Oral Health. 2024;24(1):279. doi:10.1186/s12903-024-04008-z; 38413983 DOI
- Miyayoshi Y, Hamba H, Nakamura K, Ishizuka H, Muramatsu T. Remineralization effects of enamel binding peptide, WGNYAYK, on enamel subsurface demineralization in vitro. Heliyon. 2023;10(1):e23176. doi:10.1016/j.heliyon.2023.e23176; 38148805 DOI
- Aziz S, Loch C, Li KC, Anthonappa R, Meldrum A, Ekambaram M. Remineralization potential of dentifrices with calcium sodium phosphosilicate and functionalized tri-calcium phosphate in the deeper incipient carious lesions: an in vitro study. Clin Exp Dent Res. 2024;10(2):e876. doi:10.1002/cre2.876; 38506322 DOI
- Qamar Z, Haji Abdul Rahim ZB, Neon GS, Chew HP, Zeeshan T. Effectiveness of poly-γ-glutamic acid in maintaining enamel integrity. Arch Oral Biol. 2019;106(5):104482. doi:10.1016/j.archoralbio.2019.104482; 31325718 DOI
- Qamar Z, Rahim ZBHA, Chew HP, Fatima T. Poly-γ-glutamic acid a substitute of salivary protein statherin. J Chem Soc Pak. 2016;38(4):730–6.
- Gunasekaran S, Rajan RE, Nainan PI, Sakthivel S, Varghese AA. Nanohydroxyapatite on remineralization of primary enamel lesions: a systematic review. J South Asian Assoc Pediatr Dent. 2025;8(2):126–32. doi:10.5005/jp-journals-10077-3354. DOI